Ileocaecal resection removes the terminal ileum and the caecum when they have been damaged by Crohn's disease.

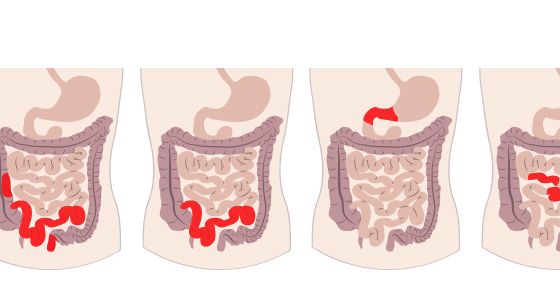
Ileocolitis - the most common type of Crohn’s disease which affects the end of the small intestine (known as the ileum) and the colon (large intestine) - most often on the right side.
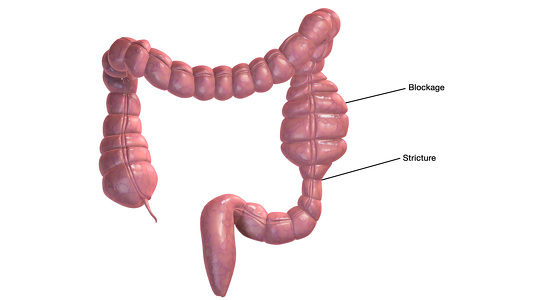
Ileocaecal resection removes the terminal ileum (the last part of the small intestine) and the caecum (the first part of the colon which connects the small and large intestines together). The healthy ends of the small intestine and the large intestine are then directly joined together. This surgery is often needed when these sections become severely damaged by Crohn’s disease. This can often result in strictures (a narrowing) of the bowel or blockages. If the strictures are long then resection surgery can be needed to remove the damaged sections. Inflammation may also cause other damage which requires them to be removed. People also have surgery if they have failed to respond to medication to help control their Crohn’s disease.
In preparation for the surgery you may be required to eat a certain diet or take certain medications or supplements to prepare your bowels. Each hospital and surgeon is different in what they require patients to do - but, for example, you may be asked to eat a low residue diet for a few days prior to your surgery and take some laxatives. Make sure you find out from your surgeon if there are any things you should/shouldn’t do to help prepare you for your operation.
Ileocaecal resection can be carried out either as open surgery or laparoscopic (keyhole) surgery.
Open surgery: You will probably be given a general anaesthetic while the operation is carried out. A catheter will be placed into your bladder to drain away urine. The surgeon will shave your abdomen and clean and prepare it using and iodine or alcohol-based cleaner. The surgeon will then make an incision in your abdomen to create an opening through which the surgery will be carried out. The terminal ileum and the caecum will be located, examined and then removed. The healthy end of the small intestine will then be attached to the healthy end of the large intestine either by staples or by being handsewn. This join is called the anastomosis.
Laparoscopic surgery: The preparation for laparoscopic surgery is similar to the open surgery above. However, instead of making one larger incision the surgeon will make several smaller incisions (or ports) through which they will work. They will use cameras, inserted through these incisions, to see what they are doing and will insert the surgical instruments and carry out the surgery through these incisions too.
In general, laparoscopic surgery results in a quicker recovery time and small scars. Sometimes, during the procedure, the surgeon discovers that it is not safe to carry out the ileocaecal resection using this technique and may have to do it through open surgery instead.
After the surgery you will probably still have a catheter in your bladder for a short time and you may also have an intravenous drip to give you fluid until you are able to drink normally again and you may also have pain medication.
Many people are encouraged to eat as soon as they feel able after the operation and are encouraged to move around too.
Generally you will need to stay in hospital for 2-5 days after laparoscopic surgery and 5-7 days for open surgery, though this can vary greatly.
After discharge from hospital you will be asked to keep mobile (moving) and avoid heavy lifting and increased physical activities for around 6 weeks. Some patients are able to begin driving again after 2 weeks, but this can vary greatly depending on the operation and the patient.