Fistulas and inflammatory bowel disease (IBD)
Fistulas are a common complication of Crohn’s disease (approximately one third of people with Crohn’s disease will develop a fistula). They are less common with ulcerative colitis.
What are fistulas?
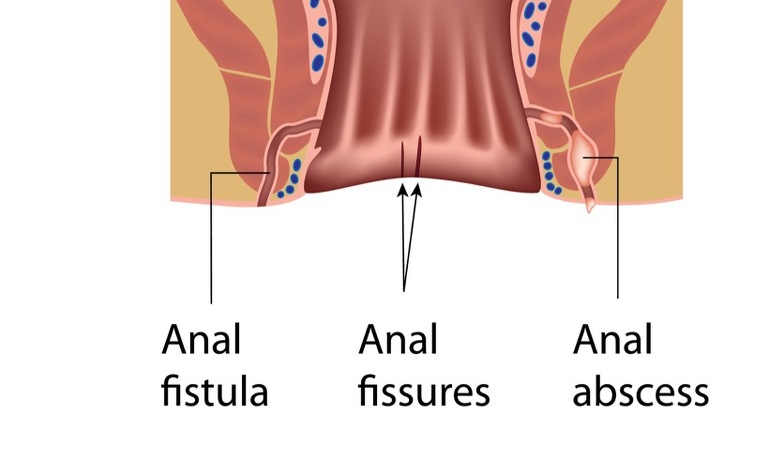
Fistulas are like tunnels which can form and connect either two different parts of the bowel together or the bowel to other organs - such as the bladder, vagina or skin. The most common site that fistula form is in the tissue surrounding the anus.
There are several different types of fistulas. These include:
- Anal or ‘perianal’ fistulas - connecting the anal canal to the surface of the skin nearby
- Enterovesicular/colovesical - bowel to bladder fistulas
- Enterovaginal - bowel to vagina fistula. If the fistula links the rectum to the vagina it is known as a rectovaginal fistula.
- Enterocutaneous - bowel to skin fistulas in areas other than near the anus, for example, on the abdomen
- Enteroenteric or enterocolic - fistulas linking different parts of the bowel or intestine together, bypassing a section in between
Who gets fistulas and why?
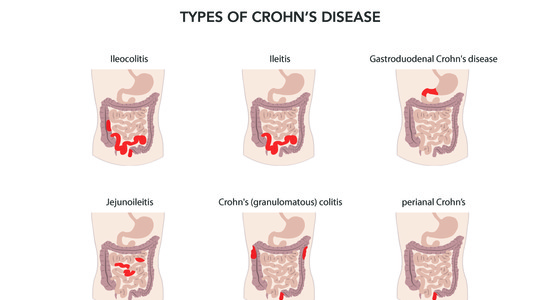
About one in three people with Crohn’s disease will probably develop a fistula at some time and the longer you have Crohn’s disease the more likely you are to develop a fistula. Fistulas are much less common in people with ulcerative colitis (UC). This is because the inflammation in Crohn’s disease tends to penetrate the whole thickness of the bowel wall. This creates ulcers, leaks and abscesses and as they develop a hole can start to form which then becomes a tunnel creating a fistula. The inflammation in UC doesn’t penetrate through the bowel wall in the same way.
Read more about how anal abscesses cause anal fistulas
What are the symptoms of fistulas?
Small fistulas may not cause any symptoms but larger ones can become infected, causing complications. This can cause a high temperature. Other symptoms vary depending on where the fistula is. They include:
- Diarrhoea and malnourishment (enteroenteric or enterocolic fistulas)
- Irritation of skin around anus, throbbing pain when you go to toilet, cough or sit in some positions and leak faeces through the fistula (anal fistulas)
- Passing wind and/or faeces through the vagina (bowel to vagina fistula)
- Leaking urine, passing air or faecal matter when urinating, frequent urge to pass urine, urinary tract infections (bowel to bladder fistulas)
It is also common to develop an abscess at the site of the fistula.
Read more about the symptoms of anal fistulas
How are fistulas diagnosed?
If your doctor suspects a fistula then they will examine your skin to see if there is a fistula visible. If one if found then they may press on the area to see if pus or faeces leaks from it. If there is no obvious fistula then you may have some tests carried out. These include:
Read more about how anal fistulas are diagnosed
How are fistulas treated?
The treatment provided will depend on the type of fistula you have and the treatment you are already receiving for your IBD. Many fistulas close following treatment and do not return. Unfortunately the treatments for fistulas aren’t always successful and you may need several treatments before the fistula heals.
Some common treatments include:
- Medical treatment via drugs such as antibiotics, immunosuppressive drug such as Azathioprine or Mercaptopurine to try to close the fistula. If these don’t work then you may be prescribed one of the biologic (or anti-TNF) drugs Infliximab or Adalimumab
- Surgical treatment. The type of surgery depends on the complexity of the fistula/s.
- Fistulotomy is a common operation used on simple low anal fistulas. The infected tract is opened and left to heal
- Seton stitch. This is used for high or complex fistulas. A soft plastic thread is threaded through the fistula and out through the anus. This helps pus or infected tissue to drain away so that the fistula can heal on its own
- Fistulectomy. The fistula is surgically removed
Read about how anal fistulas are treated