

Get IBD info delivered to your inbox
Sign up to our mailing list and receive regular articles and tips about IBD.
There are several different ways a colostomy can be performed. The specific technique used will depend on your circumstances.
The two main surgical techniques are:
Where possible, keyhole surgery is the preferred choice. This is because research has shown that patients recover quicker and have a reduced risk of complications.
However, in emergency situations, such as a bowel obstruction, the staff and equipment needed for a keyhole operation may not be available, so an open operation needs to be performed.
All colostomy procedures are carried out under general anaesthetic, which means you're asleep during surgery.
There are two main ways a colostomy can be formed:
To form a loop colostomy, a loop of colon is pulled out through an incision in your abdomen. This section of colon is opened up and stitched to the skin to form an opening called a stoma. The stoma will have two openings, but they will be close together and you may not be able to see both.
One of the openings is connected to the functioning part of your bowel. This is where waste products leave your body after the operation. The other opening is connected to the "inactive" part of your bowel, leading to your rectum. This opening only produces small amounts of mucus.
The position of the stoma depends on which section of the colon is diverted, although it's usually on the left-hand side of your abdomen, below your belt line. If the operation is planned in advance, you'll meet a specialist stoma nurse before the operation to discuss possible locations for the stoma. This may not be possible if the operation is performed as an emergency.
The stoma will appear large at first, as the effects of surgery cause it to swell. It usually shrinks during the weeks after surgery, reaching its final size after about eight weeks. The stoma will be red and moist. It has no nerve endings, so it isn't painful to touch. It may bleed when touched, but this is entirely normal and no cause for concern.
In some cases, a support device (called a rod or bridge) may be used to hold the loop of colon in place while it heals. This will usually be removed after a few days.
A loop colostomy is usually formed temporarily to treat conditions such as diverticulitis, Crohn’s disease and bowel cancer.
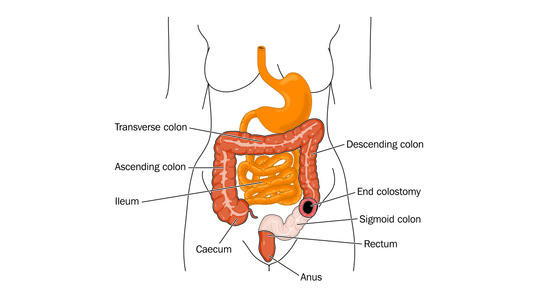
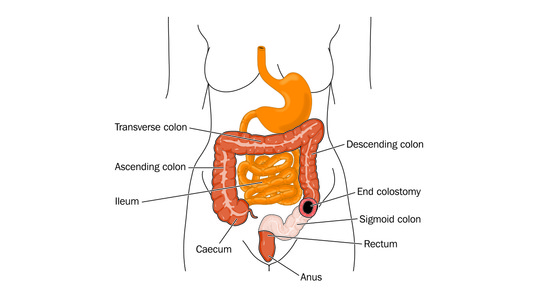
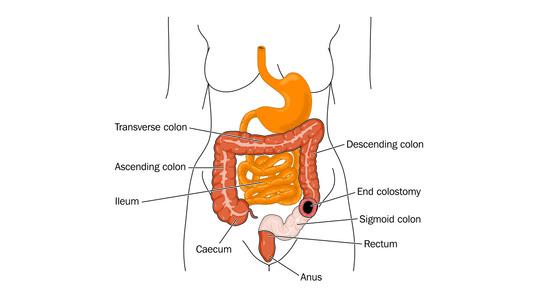
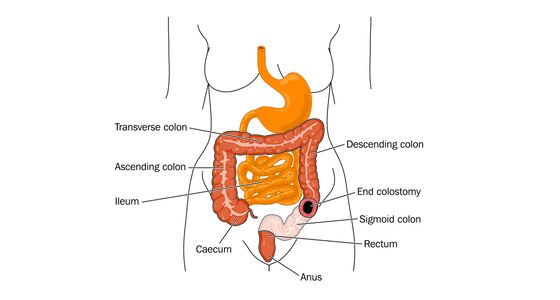
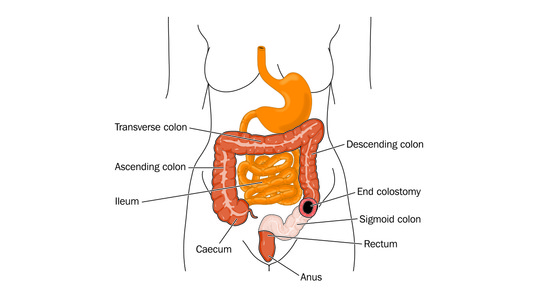
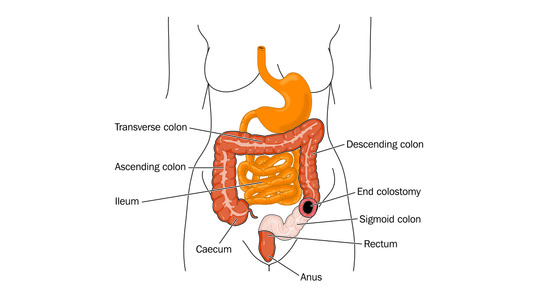
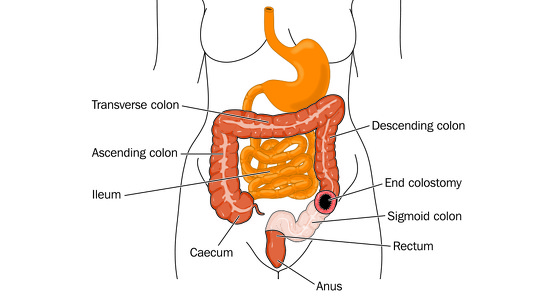
To form an end colostomy, one end of the colon is pulled out through an incision in your abdomen and stitched to the skin to create a stoma.
Like when a loop colostomy is formed, the position of the stoma depends on which section of the colon is diverted. However, it's usually on the left-hand side of your abdomen, below your belt line.
If the operation is planned in advance, you'll meet a specialist stoma nurse before the operation to discuss possible locations for the stoma. This may not be possible if the operation is performed as an emergency.
The stoma will have one opening, through which waste products pass. The other end of the colon, which goes down to your rectum, is sealed and left inside your abdomen.
End colostomies are often permanent, although temporary end colostomies are sometimes formed as an emergency to treat bowel obstructions, colon injuries or bowel cancer.
Read more about recovering from a colostomy.
In some cases, it may be possible to have an alternative procedure called an ileostomy.
This is formed in a similar way to a colostomy, but it involves diverting the small intestine instead of the large intestine.
An ileostomy may sometimes be preferable to a colostomy, because an internal pouch for waste products can be created that's connected to your anus. This can allow you to control your bowel actions in a more normal way.


Why not sign up to our mailing list and receive regular articles and tips about IBD to your inbox?