



Get IBD info delivered to your inbox
Sign up to our mailing list and receive regular articles and tips about IBD.
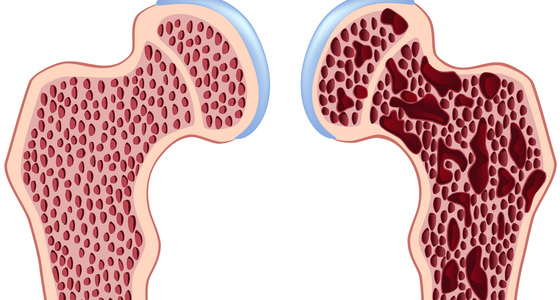
Although a diagnosis of osteoporosis is based on the results of your bone mineral density scan (DEXA or DXA scan), the decision about what treatment you need ‐ if any ‐ will also be based on a number of other factors. These include your:
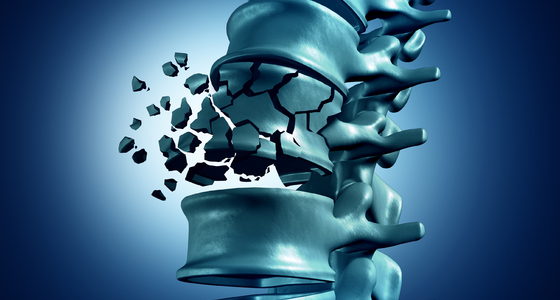
If you've been diagnosed with osteoporosis because you've had a fracture, you should still receive treatment to try to reduce your risk of further fractures.
You may not need or want to take medication to treat osteoporosis. However, you should ensure that you're maintaining sufficient levels of calcium and vitamin D. To achieve this, your healthcare team will ask you about your diet and may recommend making changes or taking supplements.
The National Institute for Health and Care Excellence (NICE) has made some recommendations about who should be treated with medication for osteoporosis.
A number of factors are taken into consideration before deciding which medication to use. These include your:
NICE has summarised its guidance for two groups of people:
You can read the NICE guidance by clicking on the links below.
A number of different medications are used to treat osteoporosis. Your doctor will discuss the treatments available and make sure the medicines are right for you.
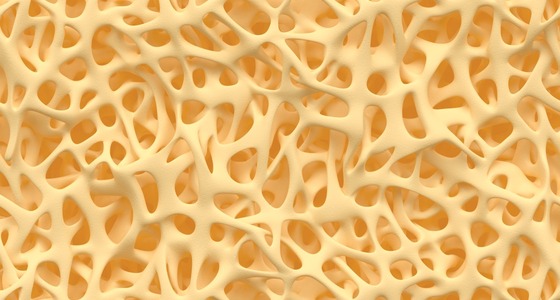
Bisphosphonates slow down the rate at which bone is broken down in your body. This maintains bone density and reduces the risk of fracture.
There are a number of different bisphosphonates, including alendronate, etidronate, ibandronate, risedronate and zolendronic acid. They're given as a tablet or injection.
You should always take bisphosphonates on an empty stomach with a full glass of water. Stand or sit upright for 30 minutes after taking them. You'll also need to wait between 30 minutes and two hours before eating food or drinking any other fluids.
Bisphosphonates usually take 6 to 12 months to work and you may need to take them for five years or longer. You may also be prescribed calcium and vitamin D supplements to take at a different time to the bisphosphonate.
The main side effects associated with bisphosphonates include:
Not everyone will experience these side effects.
Osteonecrosis of the jaw is a rare side effect that's linked with the use of bisphosphonates, although most frequently with high-dose intravenous bisphosphonate treatment for cancer and not for osteoporosis.
In osteonecrosis, the cells in the jaw bone die, which can lead to problems with healing. If you have a history of dental problems, you may need a check-up before you start treatment with bisphosphonates. Speak to your doctor if you have any concerns.
Strontium ranelate appears to have an effect on both the cells that break down bone and the cells that create new bone (osteoblasts).
It can be used as an alternative treatment if bisphosphonates are unsuitable. Strontium ranelate is taken as a powder dissolved in water.
The main side effects of strontium ranelate are nausea and diarrhoea. A few people have reported a rare severe allergic reaction to the treatment. If you develop a skin rash while taking strontium ralenate, stop taking it and speak to your doctor immediately.
Selective oestrogen receptor modulators (SERMs) are medications that have a similar effect on bone as the hormone oestrogen. They help maintain bone density and reduce the risk of fracture, particularly of the spine.
Raloxifene is the only type of SERM that's available for treating osteoporosis. It's taken as a tablet every day.
Side effects associated with raloxifene include hot flushes, leg cramps and a potential increased risk of blood clots.
Parathyroid hormone is produced naturally in the body. It regulates the amount of calcium in bone.
Parathyroid hormone treatments (human recombinant parathyroid hormone or teriparatide) are used to stimulate cells that create new bone (osteoblasts). They're given by injection.
While other medication can only slow down the rate of bone thinning, parathyroid hormone can increase bone density. However, it's only used in a small number of people whose bone density is very low and when other treatments aren't working.
Nausea and vomiting are common side effects of the treatment. Parathyroid hormone treatments should only be prescribed by a specialist.
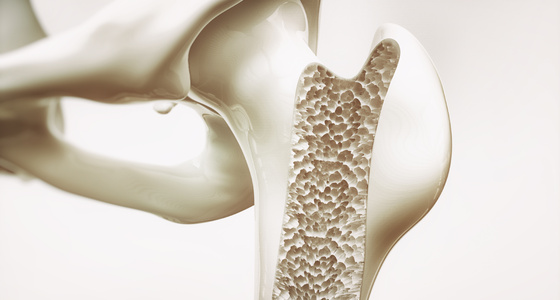
Calcium is the major mineral found in bone, and having enough calcium as part of a healthy, balanced diet is important for maintaining healthy bones.
For most healthy adults, the recommended amount of calcium is 700 milligrams (mg) of calcium a day, which most people should be able to get from a varied diet that contains good sources of calcium.
However, if you have osteoporosis you may need more calcium, which will usually be in the form of supplements. Ask your GP for advice about taking calcium supplements.
Vitamin D is needed to help the body absorb calcium. It's difficult to get enough vitamin D from your diet alone because few foods contain vitamin D. In the UK, most healthy adults obtain vitamin D from exposing the skin to summer sunlight.
However, for people at risk of not getting enough vitamin D, supplementation with 10 micrograms of vitamin D a day (400 international units (IU)) is recommended to prevent deficiency.
At risk groups include people over 65 years of age, and people who aren't exposed to much sunlight because they cover their skin for cultural reasons, are housebound, or who stay indoors for long periods.
If you're found to lack vitamin D, your GP may prescribe supplements at a higher dose than the above recommendation to correct the deficiency.
Hormone replacement therapy (HRT) is sometimes recommended for women who are experiencing the menopause as it can help control symptoms.
HRT has also been shown to maintain bone density and reduce the risk of fracture during treatment.
However, HRT isn't specifically recommended for treating osteoporosis and it isn't often used for this purpose.
This is because HRT slightly increases the risk of developing certain conditions, such as breast cancer, endometrial cancer, ovarian cancer and stroke, more than it lowers the risk of osteoporosis.
Discuss the benefits and risks of HRT with your GP.
Read more about the risks of HRT.
In men, testosterone treatment can be useful when osteoporosis is caused by insufficient production of male sex hormones (hypogonadism).
Read more about specific medicines for treating osteoporosis.


Why not sign up to our mailing list and receive regular articles and tips about IBD to your inbox?