

Get IBD info delivered to your inbox
Sign up to our mailing list and receive regular articles and tips about IBD.
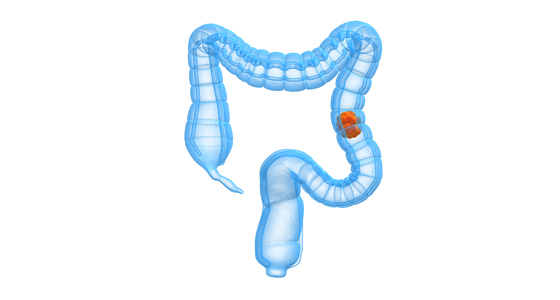
If colon cancer is at a very early stage, it may be possible to remove just a small piece of the lining of the colon wall. This is known as local excision.
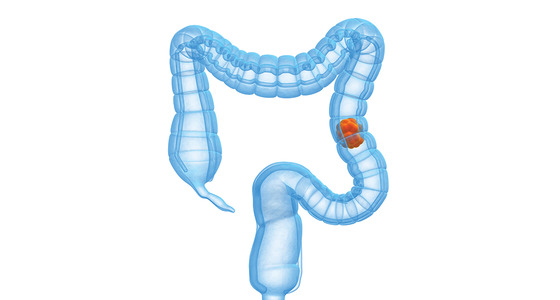
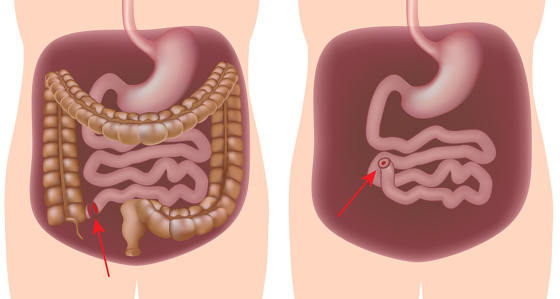
If the cancer spreads into muscles surrounding the colon, it will usually be necessary to remove an entire section of your colon. This is known as a colectomy.
There are two ways a colectomy can be performed:
During surgery, nearby lymph nodes are also removed. It is usual to join the ends of the bowel together after bowel cancer surgery, but very occasionally this is not possible and a stoma is needed.
Both open and laparoscopic colectomies are thought to be equally effective at removing cancer and have similar risks of complications.
However, laparoscopic colectomies have the advantage of a faster recovery time and less postoperative pain. It is becoming the routine way of doing most of these operations.
Laparoscopic colectomies should be available in all hospitals that carry out bowel cancer surgery, although not all surgeons perform this type of surgery. Discuss your options with your surgeon to see if this method can be used.
Want to know more?
There are a number of different types of operation that can be carried out to treat rectal cancer, depending on how far the cancer has spread.
Some of the main techniques used are described below.
If you have a very small, early-stage rectal cancer, your surgeon may be able to remove it in an operation called a local resection (transanal resection).
The surgeon puts an endoscope in through your back passage and removes the cancer from the wall of the rectum.
In many cases, however, a local resection is not possible. Instead, a larger area of the rectum will need to be removed.
This area will include a border of rectal tissue free of cancer cells, as well as fatty tissue from around the bowel (the mesentery). This type of operation is known as total mesenteric excision (TME).
Removing the mesentery can help ensure all the cancerous cells are removed, which can lower the risk of the cancer recurring at a later stage.
Depending on where in your rectum the cancer is located, one of two main TME operations may be carried out. These are outlined below.
Low anterior resection
Low anterior resection is a procedure used to treat cases where the cancer is in the upper section of your rectum.
The surgeon will make an incision in your abdomen and remove the upper section of your rectum, as well as some surrounding tissue to make sure any lymph glands containing cancer cells are also removed.
They will then attach your colon to the lowest part of your rectum or upper part of the anal canal. Sometimes they turn the end of the colon into an internal pouch to replace the rectum.
You will probably require a temporary stoma to give the joined section of bowel time to heal.
Abdominoperineal resection
Abdominoperineal resection is used to treat cases where the cancer is in the lowest section of your rectum.
In this case, it will be necessary to remove the whole of your rectum and surrounding muscles to reduce the risk of the cancer regrowing in the same area.
This involves removing and closing the anus and removing its sphincter muscles, so there is no option except to have a permanent stoma after the operation.
Bowel cancer surgeons always do their best to avoid giving people permanent stomas wherever possible.
Want to know more?
Where a section of the bowel is removed and the remaining bowel joined, the surgeon may sometimes decide to divert your stool away from the join to allow it to heal.
The stool is temporarily diverted by bringing a loop of bowel out through the abdominal wall and attaching it to the skin ‐ this is called a stoma. A bag is worn over the stoma to collect the stool.
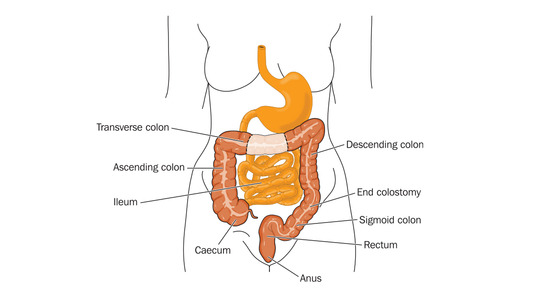
When the stoma is made from the small bowel (ileum) it is called an ileostomy, and when it is made from the large bowel (colon) it is called a colostomy.
A specialist nurse, known as a stoma care nurse, can advise you on the best site for a stoma prior to surgery.
The nurse will take into account factors such as your body shape and lifestyle, although this may not be possible where surgery is performed in an emergency.
In the first few days after surgery, the stoma care nurse will advise on the care necessary to look after the stoma and the type of bag suitable.
Once the join in the bowel has safely healed, which can take several weeks, the stoma can be closed during further surgery.
In some people, for various reasons, rejoining the bowel may not be possible or may lead to problems controlling bowel function, and the stoma may become permanent.
Before having surgery, the care team will advise you about whether it may be necessary to form an ileostomy or colostomy, and the likelihood of this being temporary or permanent.
There are patient support groups available that provide support for patients who have just had or are about to have a stoma. You can get more details from your stoma care nurse, or visit the groups online for further information.
These include:
Want to know more?
Bowel cancer operations carry many of the same risks as other major operations, including bleeding, infection, developing blood clots, or heart or breathing problems.
The operations all carry a number of risks specific to the procedure. One risk is that the joined up section of bowel may not heal properly and leak inside your abdomen. This is usually only a risk in the first few days after the operation.
Another risk is for people having rectal cancer surgery. The nerves that control urination and sexual function are very close to the rectum, and sometimes surgery to remove a rectal cancer can damage these nerves.
After rectal cancer surgery, most people need to go to the toilet to open their bowels more often than before, although this usually settles down within a few months of the operation.
There are two main ways radiotherapy can be used to treat bowel cancer. It can be given before surgery to shrink rectal cancers and increase the chances of complete removal, or be used to control symptoms and slow the spread of cancer in advanced cases (palliative radiotherapy).
Radiotherapy given before surgery for rectal cancer can be performed in two ways:
External radiotherapy is usually given daily, five days a week, with a break at the weekend. Depending on the size of your tumour, you may need one to five weeks of treatment. Each session of radiotherapy is short and will only last for 10 to 15 minutes.
Internal radiotherapy can usually be performed in one session before surgery is carried out a few weeks later.
Palliative radiotherapy is usually given in short daily sessions, with a course ranging from 2 to 3 days, up to 10 days.
Short-term side effects of radiotherapy can include:
These side effects should pass once the course of radiotherapy has finished. Tell your care team if the side effects of treatment become particularly troublesome. Additional treatments are often available to help you cope with the side effects better.
Long-term side effects of radiotherapy can include:
If you want to have children, it may be possible to store a sample of your sperm or eggs before treatment begins so they can be used in fertility treatments in the future.
Want to know more?
There are three ways chemotherapy can be used to treat bowel cancer:
Chemotherapy for bowel cancer usually involves taking a combination of medications that kill cancer cells. They can be given as a tablet (oral chemotherapy), through a drip in your arm (intravenous chemotherapy), or as a combination of both.
Treatment is given in courses (cycles) that are two to three weeks long each, depending on the stage or grade of your cancer.
A single session of intravenous chemotherapy can last from several hours to several days.
Most people having oral chemotherapy take tablets over the course of two weeks before having a break from treatment for another week.
A course of chemotherapy can last up to six months, depending on how well you respond to the treatment. In some cases, it can be given in smaller doses over longer periods of time (maintenance chemotherapy).
Side effects of chemotherapy can include:
These side effects should gradually pass once your treatment has finished. It usually takes a few months for your hair to grow back if you experience hair loss.
Chemotherapy can also weaken your immune system, making you more vulnerable to infection.
Inform your care team or GP as soon as possible if you experience possible signs of an infection, including a high temperature (fever) or a sudden feeling of being generally unwell.
Medications used in chemotherapy can cause temporary damage to men's sperm and women's eggs. This means that for women who become pregnant or for men who father a child, there is a risk to the unborn baby's health.
It is therefore recommended you use a reliable method of contraception while having chemotherapy treatment and for a period after your treatment has finished.
Want to know more?
Biological treatments, including cetuximab, bevacizumab and panitumumab, are a newer type of medication also known as monoclonal antibodies.
Monoclonal antibodies are antibodies that have been genetically engineered in a laboratory. They target special proteins found on the surface of cancer cells, known as epidermal growth factor receptors (EGFR).
As EGFRs help the cancer grow, targeting these proteins can help shrink tumours, and improve the effect and outcome of chemotherapy.
Biological treatments are therefore usually used in combination with chemotherapy when the cancer has spread beyond the bowel (metastatic bowel cancer).
These treatments are not available to everyone with bowel cancer. The National Institute for Health and Care Excellence (NICE) has specific criteria that need to be met before these can be prescribed.
Cetuximab is only available on the NHS when:
Cetuximab, bevacizumab and panitumumab are available on the NHS through a government scheme called the Cancer Drugs Fund. All these medications are also available privately, but are very expensive.
Want to know more?
Clinical commissioning groups (CCGs) are NHS bodies that organise the delivery of NHS services in England. They play a major role in achieving good health outcomes for the population they serve.
You can now check how your local CCG compares for bowel cancer survival (PDF, 900kb).


Why not sign up to our mailing list and receive regular articles and tips about IBD to your inbox?